
Child Malnutrition — The Problem looking straight into our nation’s eyes

Child malnutrition is a big blot in India’s growth story. While the world is lauding India for its growing economy, bold reforms and hordes of investors are drawn towards the world’s second largest emerging market due to its population dividend, India is fighting an internal battle to control child malnutrition and provide a healthy growth to every child.
Indian government has made some progress in this area with the help of various international organizations like UNICEF and state governments. But the results, though positive, are still far from resolving the issue completely. Indian government established a network of 1.26 million “anganwadis” (rural child care centres) that are monitored by central department like ICDS under ministry of women and child development. Each “anganwadi” centre had a workforce of 10 -15 workers to monitor 40–50 children. With this large scale workforce to monitor children, still the problem remains largely unresolved.
To write this, I have taken the approach of looking at the problem that blocks the female population of the country from being knowledgeable and aware resulting in reduction of child malnutrition. I am considering females as the focus in resolving the problem of child malnutrition because according to a pilot, Time Use Survey conducted in 18,620 households spread over six selected States, namely, Haryana, Madhya Pradesh, Gujarat, Orissa, Tamil Nadu and Meghalaya during the period June 1998 to July 1999, women spent about 2.1 hours per day on cooking food and about 1.1 hours on cleaning the households and utensils. Men’s participation in these activities was nominal. Taking care of children was one of the major responsibilities of women, as they spent about 3.16 hours per week on these activities as compared to only 0.32 hours by males.
Also, I’ll discuss the factors and root causes that plague the system and the society resulting in child malnutrition. I’ll try to depict the role of four pillars of the system, namely, Businesses (Private Sector), Government, Media and Society as a whole. But first, I’ll depict the socio economic factors first before I get into how the four pillars can actually do something.
Note : All the data points are referenced from various sources which are mentioned at the end of this article. but the opinion is completely personal.
Malnutrition in India — A Quick Snapshot
The state of hunger and malnutrition in India is worrying. India has the highest number (one quarter) of undernourished (hungry) people in the world (194.6 million or 15 percent of India’s total population during 2014–16). Hunger and undernourishment lead to severe problems. Children and youth in this state suffer from numerous nutritional deficiencies which adversely impact their overall health. In India, data for 2015–16 show the following:
-
38 percent of children below five years (urban: 31%, rural: 41%) are stunted (low height for age);
-
21 percent (urban: 20%, rural: 22%) are wasted (low weight for height);
-
36 percent (urban: 29%, rural: 38%) are underweight (low weight for age);
-
2 percent were overweight in 2006 (above normal weight for height); and
-
58 percent of children aged between 6 and 59 months (urban: 56%, rural: 59%) are anaemic.
Malnutrition in children under-five also results in nearly half of the 1.3 million deaths occurring in the country each year.
India Against Child Malnutrition — the story so far
To understand any problem landscape in India, India is always divided in two segments : Rural and Urban. That is because gap between the two is so large that hypothetically, they can be separated in a logical zone and they can even form two separate economies of its own.
With a total population of approximately 1.3 billion, rural india has a female population of 405.83 million and male population of 427.63 million. While urban india has a female population of 181.62 million and male population of 192.49 million. Now, with the base numbers in place, we can evaluate the socio-economic factors of females in India. Because if the mother knows the importance of health and nutrition and keeps herself healthy, the child will never suffer from malnutrition.
The Education Factor
Before moving to any other factor, let’s discuss the education levels of females in India. There is a big difference in being literate and being educated. India’s literacy numbers on the rise but then, the same growth in literacy should have resulted in awareness of health care of self and the child in females. If that is not being reflected in the data, it means literacy is not helping directly in the education or knowledge levels of the significant female population. Let’s compare the following two data tables (Figure 1 and Figure 2).
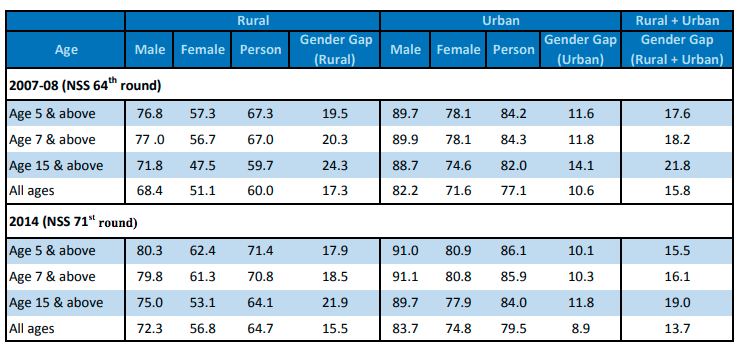
Figure 1 : Literacy rates (%) for persons in different age-groups for rural & urban population as per NSS
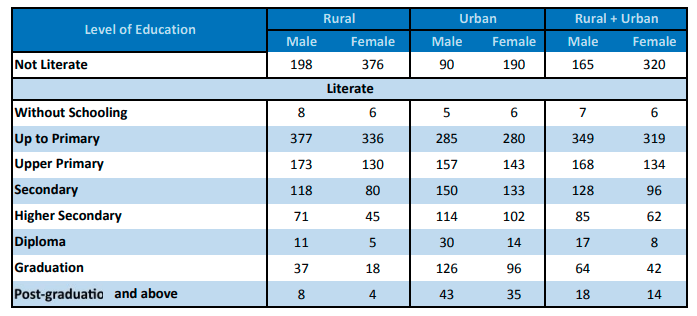
Figure 2 : Per 1000 distribution of persons (aged 5 years and above) by completed level of education : 2014
By looking at the above data tables, it is easily noticeable that even thought literacy rate gone significantly up for females, most of it is contributed to the fact that enrolment of females is highest at primary level and declines significantly after that. Going to school does make females literate but it still does not help them being aware of health factors that result in child malnutrition in later part of their life.
Education is a significant factor in creating knowledge and awareness. If the number of females going to secondary school level is increased significantly, it can help creating awareness of health related issues. But then, it’s not by choice that females drop out of education system.
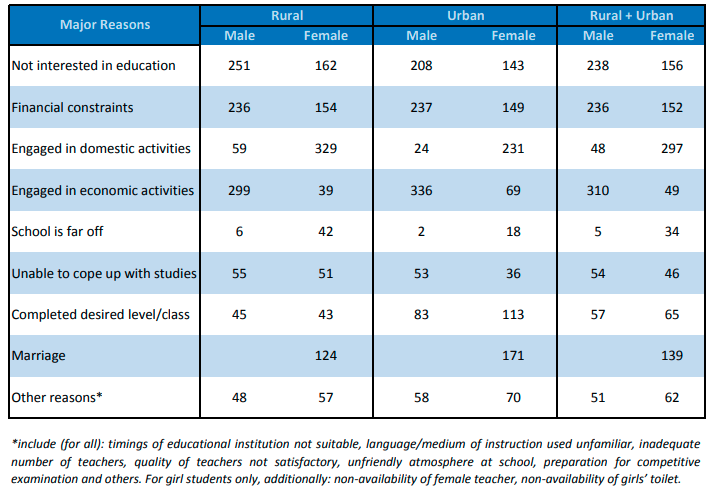
Figure 3: Per 1000 distribution of dropping out/discontinuance (for persons aged 5–29 years) by reasons for dropping out/discontinuance : 2014
The above given table depicts the causes why there is high drop rate of females from the education system.In this case, Rural and urban is not making much of a difference. This means there are various other factors like economic, geographical location and social status of the family including caste and religious beliefs that contribute to females being less aware of the health of oneself and the child.
The Economic Factor
In 2011, the Workforce Participation Rate at all India level was 25.51% for females and 53.26% for males. While there is no rural — urban gap for males (53%), there is considerable rural — urban gap for females (rural -30%, urban- 15.4%). Workforce Participation rate for females is significantly higher at 41.8% in rural areas against urban participation rate of 35.31%.
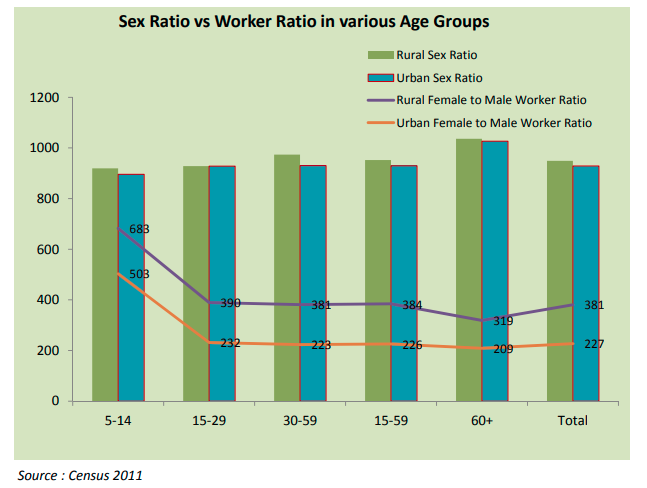
Figure 4 : Sex Ratio vs Worker Ratio in various age groups
Let’s look at the above chart. This depicts at the age group of 5–14, 683 females are part of workforce in India as compared to 1000 males. Now, both males and females at this age group should be in school but due to poor economic condition of the family, they end up being a part of majorly unskilled workforce. This results in lower rate of admission in schools and hence, a very low rate of awareness about health factors.
The Social ( Caste and Religion ) Factor
Even when we are in 21st century and India celebrated its 70 years of independence in 2017, India still has very strong caste and religion based culture making sure of economic exclusion and disparity for females resulting in low education and economic growth and indirectly, resulting in child malnutrition due to religious preferences. According to Planning Commission statistics for 2009–10, in urban areas, ST and SC have a poverty rate of 30.4% and 34.1% respectively compared to 12.4% for Hindus and 21% for India as a whole. Similarly in rural areas, compared to an overall poverty rate of 33.8%, ST and SC have a head count ratio (HCR) of 47.4% and 42.3% respectively (Government of India, 2012). Muslim women have largely been absent from realm of economic enquiry. With a large population divided on the basis of caste and religion, economic sufficiency resulting in higher rate of education levels become difficult.
The Health Factor
If we take into account all the above factors (Education, Economic and Social), the health factor becomes low obvious on the priority order of females. To depict that, let’s examine following data table depicting fertility rates as per the education level of the females
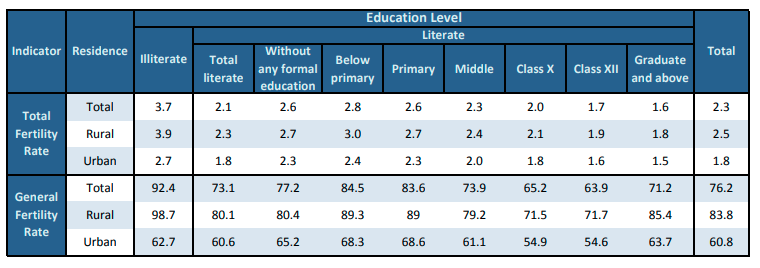
Figure 5 : Fertility indicators by level of education of women, 2015
In the above data, the total fertility rate of illiterate rural females is as high as 3.9 and 2.7 in urban females. While, for the females who are graduate and above, fertility rate in both rural and urban section is 1.8 and 1.5 respectively. If we examine it closely, till middle level education, fertility rate remains high on an average of approximate 2.6. To derive a conclusion, due to lower education levels and social pressures due to caste and religion, females are giving birth to more number of children. As number of children per family grow but per capita income does not increase significantly, it results in less allocation of resources per child and hence, resulting in malnutrition for many of the children in the family.
India Against Child Malnutrition — Going Forward
While India as a whole has its own political, economical and social limitations to bring a significant reduction in child malnutrition if not completely resolve it, various sections of India can play their role independently to help in containing this problem. And if all of these multiple sections (private sector, government, society, media and international social organizations) work in collaboration, then the problem of child malnutrition may completely be resolved that it becomes an insignificant problem.
Role of Government
Indian government has been concerned about child malnutrition to a good extent. So much so, that , it finds the space in the finance minister’s budget speech every year and that too, as the first action item. Following figure depicts the allocation of amount to ICDS (Integrated Child Development Services) in annual budget every year.
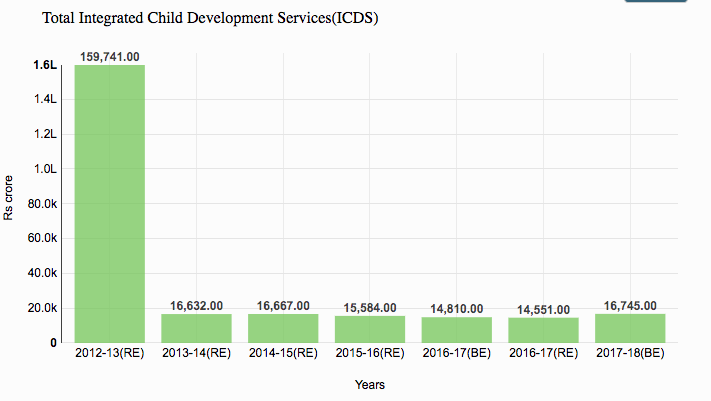
Figure 6 : Budgetary Allocation Figures for Integrated Child Development Services(ICDS) includes ICDS core; National Nutrition Mission and World Bank assisted ICDS.
This budgetary allocation is even less than 0.5% of total annual budget of Indian government. And in other terms, it is less than 0.1% of India’s GDP.
Indian government started a wonderful concept of “aanganwadi” centers way back in 1975 and the goal was to provide basic health care and nutrition to every child. This programme has worked great and expanded over a period of time proving its success by bringing down the child malnutrition ratios. But the government has to play much more active role by adhering to its responsibility and accountability towards child malnutrition apart from just allocation of budget.
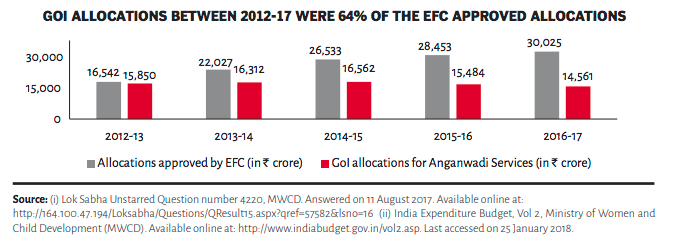
Figure 7 : GOI allocations between 2012–17 were 64% of the EFC approved allocations
Even if the government allocates the budget, Expenditure Finance Committee (EFC) approved only 64% of the total amount. That resulted in less money at the disposal of Anganwadi centers and hence, the lower performance results.
Another issue happens at state / local government level. From the below chart of states, it is obvious that even with the money at their disposal, the execution of the whole programme done by some of the states is not efficient resulting in vacant positions and un-operational health care or aaganwadi centers. As per government plan, the Anganwadi Centre (AWC) is the first point of service delivery for health, nutrition and early learning for children at the village level. But as on 30 September 2017, of the 14 lakh sanctioned AWCs, 13.59 lakh (97 per cent) were operational. Many existing AWCs do not have required facilities. For instance, as on September 2016, only 70 per cent of AWCs/ mini-AWCs had drinking water facilities and only 63 per cent had toilet facilities
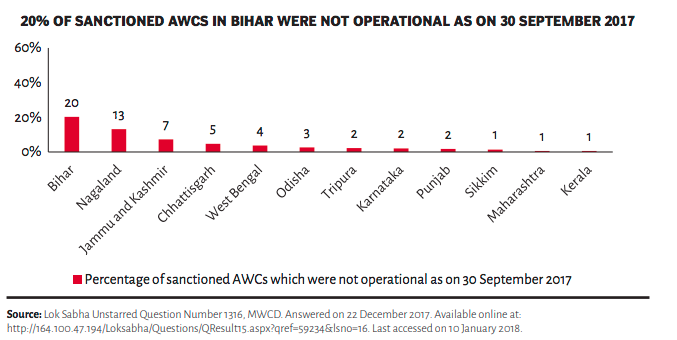
Figure 8 : Percentage of sanctioned AWCs which were not operational as on 30th September 2017
These are just few of the many instances that the government need to look at. Not only allocation of significant budget for the cause of child malnutrition, the government needs to look the whole execution workflow including the availability of people, resources, physical infrastructure and transport among other things. To do all of this, a very influential, responsible and accountable hierarchy has to be in place so that in case of deficiency of service, appropriate action can be taken.
Role of Private Sector
Corporate Sector is as important in the resolution of the large scale issues like these as the government. For this reason, government made it mandatory for private sector organizations to pay 2% of their net profit to social organisations as Corporate Social Responsibility (CSR). This was even made tax free so that it is done by corporate sector in a genuine manner and it will fund the social sector organizations and in turn, reduce the dependency on government grants. While this is a great scheme, private sector has never done enough. One may argue that child malnutrition is a government subject, while I argue that private sector shall play an equally important role. After all, the workforce that works in the private sector is the one that has children suffering from malnutrition. And if the child is suffering, parent cannot be highly productive.
More than driven by data, the role of private sector is philosophical. For profit organizations can offer their technology, research experience and expertise for the cause of child malnutrition. For instance, data gathering is one of the biggest problems in reducing the child malnutrition in India. Private sector technology companies can effectively solve the data gathering problem by the use of last mile in-expensive technology and devices while enabling data analytical tools to facilitate smooth operations of the whole ICDS program. It’s not that government is not willing to pay for it, but private sector has to take the lead in building such systems. When facebook has reached in every hand in India due to penetration of cellphones, posting simple data like height, weight and nutritional statistics becomes so simple.
Also, private sector can help contain the problem of food wastage so that more food is made available to the people who need it. According to IFPRI, just a 10% reduction in food wastage can help in bring down the prices of food available in the market by 14%. Private sector organizations dealing in the food and agricultural sector can help the farmers grow food with more nutritional content. This does not mean that any private sector company shall compromise on their profit goals but they can align the profit goals with technology research and support that is required to eradicate the problem of child malnutrition.

Figure 9 : healthphone.org , in partnership with Vodafone.
HealthPhone (http://iap.healthphone.org/) is one of the perfect example where a corporate sector company partnered with government and international organization like UNICEF to build solutions in helping reduce child malnutrition in India.
Role of Media
Media has a very significant role to play in the reduction of child malnutrition. Media is not only about news channels or newspapers, it’s about the content people watch on television, listen on radio and read in books, magazines and newspapers. Time and again, media has played a crucial role in reaching out to masses for information dissemination. While the government does its job by employing the services of the media owned and operated by them (like doordarshan), even private media companies need to share the responsibility.
It’s true media organizations shall maintain their journalistic integrity and follow the story but they should follow the story sometimes, not only to criticise every effort of the government but even to laud the efforts of the officials working hard in resolving the issues.
Media has the power to disseminate the information with the use of celebrities to inform people about dietary requirements of a child and mother, sanitary and hygiene, informing about prevention of diseases and treatments that are non-invasive and in-expensive and even dispel the myths and taboos of various food items and their related nutrient values.
For instance, India has been successful in eradicating Polio completely by 2015 after humongous efforts by the government. Media was instrumental in running campaigns across the country in both print and electronic medium. With getting celebrities on-board, they were effective in communicating the message to the people and guide them to the right solution.
Media is the one that can create awareness and knowledge. For example, television channels organizes TV shows like “Satyamev Jayate” which focuses on making people aware of the harsh realities of life. It mainly discusses and provides possible solutions relating to the various social issues of India. It aims to empower citizens with informations. Hence, through this type of shows, many NGOs comes up with the social causes and holds campaigns, demonstration, and protests in order to demand justice.
Role of Society
Society, at large, has been always on the receiving side. It’s a faceless gathering of people that just wants to take everything from every source without giving anything back. Historically, societies have never changed on their own without a push from governments and from the fear of social boycotts.
Having a male child has been more important for most of the indians than the female child. If we have look at the data table below, it depicts that 45% of the mothers still want a male child. The reason of this want can be many including domestic abuse, social pressure or anything else.
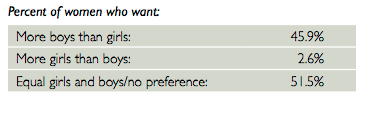
Figure 10 : Percentage of women who want boy than girl
If the girl child is born (as if it’s in control of humans), then she is not taken care of as she should be. This results in the malnutrition of the girl child. For instance, even in 21st century that we live in, female child has higher chances of malnutrition that male child. The next data chart indicates the same.
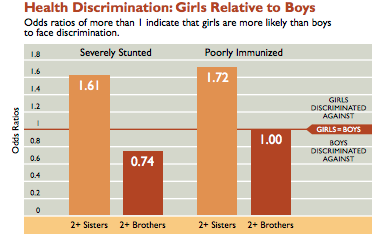
Figure 11: Health discrimination between girls and boys
The gender discrimination is one of the causes of child malnutrition. Not only the child, but because of the gender discrimination, even mothers remain under-nourished. As per latest NFHS-4 survey, girl child is fed less time on breast milk as compared to boys.
Society cannot change overnight but the collaboration of all the other three (private sector, government and media) can bring a change faster if they wish to.
Conclusion
Child malnutrition is a large scale issue for India. But it can only be solved effectively when all the four pillars of this ecosystem (government, media, private sector and society) come together and work in tandem.
One of the most important aspects of solving the problem will be getting accurate data and then, updating it on regular intervals to get the right measurements. In most of the cases, even if everyone works together but the data collected is incorrect, the problem just grows manifold instead of getting reduced.
The problem of child malnutrition should be taken at a war scale. Because, these children are the future of this country and we cannot afford to have a malnourished future.
References
-
Report on Women and Men in India — 2017 by Ministry of statistics and programme implementation . (http://www.mospi.gov.in/publication/women-and-men-india-2017)
-
Religion, Literacy, and the Female-to-Male Ratio in India — Vani K. Borooah and Sriya Iyer ( https://pdfs.semanticscholar.org/deff/d944641237716d40f143bd211cb67133fe60.pdf )
-
Union Budget Analysis Tool — 2017–2018 ( http://unionbudget2017.cbgaindia.org/budget_overview/index.html )
-
Poshan ( http://iap.healthphone.org/ )
-
2016 Global Food Policy Report by IFPRI ( http://ebrary.ifpri.org/cdm/ref/collection/p15738coll2/id/130207 )
-
Son Preference and Daughter Neglect in India — Rohini Pandey and Anju Malhotra ( https://www.unfpa.org/sites/default/files/resource-pdf/UNFPA_Publication-39764.pdf )
-
Nutrition in India : Targeting the first 1000 days of a child’s life — Shamika Devi , Ramandeep Singh ( https://www.brookings.edu/wp-content/uploads/2016/10/20161023_policybrief_2.pdf )
-
India : Nutrition Profile — FantaProject.org ( https://www.fantaproject.org/sites/default/files/download/India-Nutrition-Profile-Mar2014.pdf )
-
Preventing hunger and malnutrition in India — Rumi Aijaz ( https://www.orfonline.org/research/preventing-hunger-and-malnutrition-in-india/ )
-
Annual Health Survey Report — Ministry of home affairs ( http://www.censusindia.gov.in/vital_statistics/AHS/AHS_report_part2.pdf )
-
Nutrition data of Indian states and districts — Niti Aayog ( http://niti.gov.in/content/nutrition-charts )
-
UNICEF data — monitoring the situation of children and women ( https://data.unicef.org/country/ind/ )